The The Space Shuttle Columbia disaster was
the disintegration of the Space Shuttle Columbia over Texas on February 1,
2003, during re-entry into the Earth's atmosphere on its 28th mission,
STS-107. The entire seven-member crew died.
The loss of the Columbia was caused by damage sustained during launch when
most of the left bipod foam ramp (see below) broke off the main propellant
tank under the aerodynamic forces of launch and struck the orbiter's left
wing leading edge. A thermal protection system (TPS) panel on the wing was
damaged, which allowed the hot gasses of re-entry to penetrate and weaken
the wing structure, ultimately causing it to fail. The vehicle became
uncontrollable and was destroyed by the extreme heat of re-entry.
Some engineers suspected damage to the thermal protection, but NASA
managers limited the investigation, feeling that nothing could be done
even if damage was found.
U.S. manned space flights did not resume until over two years later, but
the foam shedding problem continued. Despite these setbacks, the
International Space Station continues to operate with a skeleton crew
transported and supplied by Russian space vehicles.
There have now been two such losses of a space shuttle and crew. The first
was the Challenger disaster in 1986.
Crew

The crew of STS-107 on launch day
Commander: Rick D. Husband, a US Air
Force colonel and mechanical engineer, who piloted a previous shuttle
during the first docking with the International Space Station.
Pilot: William C. McCool, a US Navy commander
Payload Commander: Michael P. Anderson, a US Air Force lieutenant
colonel and physicist who was in charge of the science mission.
Payload Specialist: Ilan Ramon, a colonel in the Israeli Air Force
and the first Israeli astronaut.
Mission Specialist: Kalpana Chawla, an Indian-born aerospace
engineer on her second space mission.
Mission Specialist: David M. Brown, a US Navy captain trained as an
aviator and flight surgeon. Brown worked on a number of scientific
experiments.
Mission Specialist: Laurel Clark, a US Navy captain and flight
surgeon. Clark worked on a number of biological experiments.
Debris strike during launch
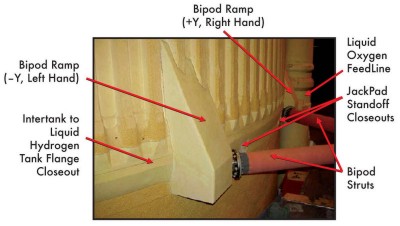
Close-up of the Left Bipod Foam Ramp that broke off and damaged the
Shuttle wing.
STS-107 had been delayed 18 times over the
course of two years (despite its designation as the 107th mission, it was
actually the 113th mission launched) from its original launch date of 11
January 2001 to its actual launch date of 16 January 2003. A
well-publicized launch delay due to cracks in the shuttle's propellant
distribution system occurred one month before a 19 July 2002 launch date,
but the Columbia Accident Investigation Board (CAIB) determined that this
delay had nothing to do with the catastrophic failure six months later.

Columbia lifting off on its final mission. The light-coloured triangle
visible at the base of the strut is the Left Bipod Foam Ramp.
The Left Bipod Foam Ramp is an approximately
three-foot (one-metre) piece made entirely out of foam, as opposed to
being a metal ramp that is merely coated with foam. As such, the foam, not
normally considered to be a structural material, is required to bear some
aerodynamic loads. Because of these special requirements, the
casting-in-place and curing of the ramps may be performed only by a senior
technician. Apparently, even the best technical servicing available could
not compensate for this fatal design flaw.
Bipod Foam Ramps had fallen off on at least three previous Shuttle
flights, with at least one previous Shuttle strike but no serious damage.
The euphemism used by NASA management to refer to this phenomenon was
"foam shedding." As with the O-ring erosions that ultimately doomed the
Challenger Shuttle, NASA management seemed to grow complacent and
accustomed to these phenomena when no serious consequences resulted from
these earlier episodes.
Video taken during lift-off was routinely reviewed two hours after the
launch and revealed nothing unusual. The following day, higher-resolution
film that had been processed overnight revealed that a piece of insulation
foam fell from the external fuel tank 81.9 seconds after launch and
appeared to strike the shuttle's left wing, potentially damaging the
thermal protection on the Space Shuttle. The exact location where the foam
struck the wing could not be determined due to the low resolution of the
tracking camera footage.
Launch to Landing
In a risk-management scenario similar to the
Challenger disaster, NASA management failed to recognize the relevance of
engineering concerns for safety. Two examples of this were failure to
honour engineer requests for imaging to inspect possible damage, and
failure to respond to engineer requests about status of astronaut
inspection of the left wing.
Engineering made three separate requests for Department of Defence (DOD)
imaging of the shuttle in orbit to more precisely determine damage. While
the images were not guaranteed to show the damage, the capability existed
for imaging of sufficient resolution to provide meaningful examination. In
fact the Columbia Accident Investigation Board (CAIB) recommended
subsequent shuttle flights be imaged while on orbit using ground-based or
space-based Department of Defence assets [1]. NASA management did not
honour the requests and in some cases intervened to stop DOD from
assisting.
NASA's chief thermal protection system (TPS) engineer was concerned about
left wing TPS damage and asked NASA management whether an astronaut would
visually inspect it. NASA managers never responded.
Throughout the risk assessment process, senior NASA managers were
influenced by their belief nothing could be done even if damage was
detected, hence this affected their stance on investigation urgency,
thoroughness and possible contingency actions. They decided to conduct a
parametric "what-if" scenario study more suited to determine risk
probabilities of future events, instead of inspecting and assessing the
actual damage.
Much of the risk assessment hinged on damage predictions to the thermal
protection system. These fall into two categories: damage to the silica
tile on the wing lower surface, and damage to the reinforced carbon/carbon
leading edge panels.
Boeing-developed damage prediction software was used to evaluate possible
tile and reinforced carbon/carbon (RCC) damage. The software predicted
severe penetration of multiple tiles by the impact, but Boeing engineers
downplayed this. They believed that results showing that the software
overstated damage from small projectiles meant that the same would be true
of larger foam (SOFI) impacts. The program used to predict RCC damage was
based on small ice impacts, not larger SOFI impacts. Under 1 of 15
predicted SOFI impact paths, the software predicted an ice impact would
completely penetrate the RCC panel. Engineers downplayed this, too,
believing that impacts of the less dense SOFI material would result in
less damage than ice impacts. In an e-mail exchange, NASA managers
questioned whether the density of the SOFI could be used as justification
for reducing predicted damage. Despite engineering concerns about the
energy imparted by the SOFI material, NASA managers ultimately accepted
the rational to reduce predicted damage of the RCC panels from complete
penetration to slight damage to the panel's thin coating.
NASA managers assumed a rescue or repair was impossible, so there was no
point in trying to inspect the vehicle for damage while on orbit. However
the CAIB determined either a rescue mission or on-orbit repair, though
risky, might have been possible had NASA verified severe damage within
five days into the mission.
Ultimately the NASA Mission Management Team felt there was insufficient
evidence to indicate that the strike was an unsafe situation, so they
declared the debris strike a "turnaround" issue (not of highest
importance) and denied the requests for the Department of Defence images.
Destruction during re-entry
At 2:30 a.m. EST on February 1, 2003, the
Entry Flight Control Team began duty in the Mission Control Centre. The
Flight Control Team was not working on any issues or problems related to
the planned de-orbit and re-entry of Columbia. In particular, the team
indicated no concerns about the debris impact to the left wing during
ascent, and treated the re-entry like any other. The team worked through
the de-orbit preparation checklist and re-entry checklist procedures.
Weather forecasters, with the help of pilots in the Shuttle Training
Aircraft, evaluated landing-site weather conditions at the Kennedy Space
Centre. At the time of the de-orbit decision, about 20 minutes before the
initiation of the de-orbit burn, all weather observations and forecasts
were within guidelines set by the flight rules, and all systems were
normal.
Shortly after 8:00 a.m., the Mission Control Centre Entry Flight Director
polled the Mission Control room for a GO/NO-GO decision for the de-orbit
burn, and at 8:10 a.m., the Capsule Communicator notified the crew they
were GO for de-orbit burn.
As the Orbiter flew upside down and tail-first over the Indian Ocean at an
altitude of 175 statute miles (282 km), Commander Husband and Pilot McCool
executed the de-orbit burn at 8:15:30 a.m. using Columbia’s two Orbital
Manoeuvring System engines. The de-orbit manoeuvre was performed on the
255th orbit, and the 2-minute, 38-second burn slowed the Orbiter from
17,500 mph (7.8 km/s) to begin its re-entry into the atmosphere. During
the de-orbit burn, the crew felt about 10% of the effects of gravity.
There were no problems during the burn, after which Husband manoeuvred
Columbia into a right-side-up, forward-facing position, with the Orbiter’s
nose pitched up.
Entry Interface, arbitrarily defined as the point at which the Orbiter
enters the discernible atmosphere at 400,000 feet (120 km), occurred at
8:44:09 a.m. (Entry Interface plus 000 seconds, written EI+000) over the
Pacific Ocean. As Columbia descended from space into the atmosphere, the
heat produced by air molecules colliding with the Orbiter typically caused
wing leading-edge temperatures to rise steadily, reaching an estimated
2,500 degrees Fahrenheit (1400 °C) during the next six minutes. As
superheated air molecules discharged light, astronauts on the flight deck
saw bright flashes envelop the Orbiter, a normal phenomenon.
At 8:48:39 a.m. (EI+270), a sensor on the left wing leading edge spar
showed strains higher than those seen on previous Columbia re-entries.
This was recorded only on the Modular Auxiliary Data System, and was not
telemetered to flight controllers or displayed to the crew.
At 8:49:32 a.m. (EI+323), travelling at approximately Mach 24.5, Columbia
executed a roll to the right, beginning a pre-planned banking turn to
manage lift, and therefore limit the Orbiter’s rate of descent and
heating.
At 8:50:53 a.m. (EI+404), travelling at Mach 24.1 and at approximately
243,000 feet (74 km), Columbia entered a 10-minute period of peak heating,
during which the thermal stresses were at their maximum. By 8:52:00 a.m.
(EI+471), nearly eight minutes after entering the atmosphere and some 300
miles (500 km) west of the California coastline, the wing leading-edge
temperatures usually reached 2,650 degrees Fahrenheit (1450 °C). Columbia
crossed the California coast west of Sacramento at 8:53:26 a.m. (EI+557).
Travelling at Mach 23 and 231,600 feet (70.6 km), the Orbiter’s wing
leading edge typically reached more than an estimated 2,800 degrees
Fahrenheit (1540 °C).

Columbia at approximately 0857. Debris is already starting to come off
from the left wing.
On crossing California, the Orbiter appeared
to observers on the ground as a bright spot of light moving rapidly across
the sky. Signs of debris being shed were sighted at 8:53:46 a.m. (EI+577),
when the superheated air surrounding the Orbiter suddenly brightened,
causing a noticeable streak in the Orbiter’s luminescent trail. Observers
witnessed another four similar events during the following 23 seconds, and
a bright flash just seconds after Columbia crossed from California into
Nevada airspace at 8:54:25 a.m. (EI+614), when the Orbiter was travelling
at Mach 22.5 and 227,400 feet (69.3 km). Witnesses observed another 18
similar events in the next four minutes as Columbia streaked over Utah,
Arizona, New Mexico, and Texas.
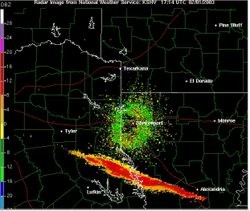
Columbia debris (in red, orange, and yellow) detected by National Weather
Service radar over Texas and Louisiana
In Mission Control, re-entry appeared normal
until 8:54:24 a.m. (EI+613), when the Maintenance, Mechanical, and Crew
Systems (MMACS) officer informed the Flight Director that four hydraulic
sensors in the left wing were indicating “off-scale low,” a reading that
falls below the minimum capability of the sensor. As the seconds passed,
the Entry Team continued to discuss the four failed indicators.
At 8:55:00 a.m. (EI+651), nearly 11 minutes after Columbia had re-entered
the atmosphere, wing leading-edge temperatures normally reached nearly
3,000 degrees Fahrenheit (1650 °C). At 8:55:32 a.m. (EI+683), Columbia
crossed from Nevada into Utah while travelling at Mach 21.8 and 223,400 ft
(68 km). Twenty seconds later, the Orbiter crossed from Utah into Arizona.
At 8:56:30 a.m. (EI+741), Columbia initiated a roll reversal, turning from
right to left over Arizona. Travelling at Mach 20.9 and 219,000 feet,
Columbia crossed the Arizona-New Mexico state line at 8:56:45 (EI+756),
and passed just north of Albuquerque at 8:57:24 (EI+795).
Columbia debris (in red, orange, and yellow) detected by National Weather
Service radar over Texas and Louisiana. Around 8:58:00 a.m. (EI+831), wing
leading-edge temperatures typically decreased to 2,880 degrees Fahrenheit
(1580 °C). At 8:58:20 a.m. (EI+851), travelling at 209,800 feet (64 km)
and Mach 19.5, Columbia crossed from New Mexico into Texas, and about this
time shed a Thermal Protection System tile, which was the most westerly
piece of debris that has been recovered. Searchers found the tile in a
field in Littlefield, Texas, just northwest of Lubbock. At 8:59:15 a.m.
(EI+906), MMACS informed the Flight Director that pressure readings had
been lost on both left main landing-gear tires. The Flight Director then
told the Capsule Communicator (CAPCOM) to let the crew know that Mission
Control saw the messages and was evaluating the indications, and added
that the Flight Control Team did not understand the crew’s last
transmission.
At 8:59:32 a.m. (EI+923), a broken response from the mission commander was
recorded: “Roger, uh, bu - [cut off in mid-word] …” It was the last
communication from the crew and the last telemetry signal received in
Mission Control. Videos made by observers on the ground at 9:00:18 a.m.
(EI+969) revealed that the Orbiter was disintegrating.
At about 9:05 (14:05 UTC), residents of north central Texas reported a
loud boom, a small concussion wave and smoke trails and debris in the
clear skies above the counties southeast of Dallas. More than 2,000 debris
fields, as well as human remains, were found in sparsely populated areas
southeast of Dallas from Nacogdoches in East Texas, where a lot of debris
fell, to western Louisiana and the south-western counties of Arkansas.
This debris included live C. elegans worms from a science package that
survived the re-entry. NASA issued warnings to the public that any debris
could contain hazardous chemicals, that it should be left untouched, its
location reported to local emergency services, or government authorities
and that anyone in unauthorized possession of debris would be prosecuted.
Shortly after being told of reports of pieces of the shuttle being seen to
break away, the NASA flight director declared a contingency (events
leading to loss of the vehicle) and alerted search and rescue teams in the
area. He told the ground controller to "lock the doors", which is the code
phrase that a contingency is in effect, nobody can enter or leave the
room, and flight controllers should preserve all the mission data for
later investigation.
Initial investigation
NASA Space Shuttle Program Manager Ron
Dittemore reported that "The first indication was loss of temperature
sensors and hydraulic systems on the left wing. They were followed seconds
and minutes later by several other problems, including loss of tire
pressure indications on the left main gear and then indications of
excessive structural heating". Analysis of 31 seconds of telemetry data
which had initially been filtered out because of data corruption within it
showed the shuttle fighting to maintain its orientation, eventually using
maximum thrust from its reaction control system jets.
The focus of the investigation centred on the foam strike from the very
beginning. Incidents of debris strikes from ice and foam causing damage
during take-off were already well known, and had actually damaged orbiters,
most noticeably during STS-45, STS-27, and STS-87 [8]. Tile damage had
also been traced to ablative insulating material from the solid rocket
motors in the past. The composition of the foam insulation had been
changed in 1997 to exclude the use of Freon, a chemical that causes ozone
depletion; while NASA was exempted from legislation phasing out CFCs, the
agency chose to change the foam nonetheless. This led to many statements
linking the foam strike to environmental pressures. STS-107 used an older
"lightweight tank" where the foam was sprayed on to the larger cylindrical
surfaces using the newer no freon foam. However the bipods were
manufacture red from BX-250 foam which was excluded from the EPA
regulations and did use the original Freon formula. The composition change
did not contribute to the accident.
Was rescue or repair
possible?
Had NASA management acted in time, two
possible contingency procedures were available: A rescue mission by
shuttle Atlantis, and an emergency spacewalk to attempt repairs to the
left wing thermal protection.
Rescue
The CAIB determined a rescue mission, though risky, might have been
possible provided NASA management took action soon enough.
Normally a rescue mission isn't possible, due to the time required to
prepare a shuttle for launch, and the limited consumables (power, water,
air) of an orbiting shuttle. However in this case Atlantis was well along
in processing for a March 1 launch. Also Columbia carried an unusually
large quantity of consumables due to an Extended Duration Orbiter (EDO)
package. This would have allowed Columbia to stay in orbit until flight
day 30 (February 15). NASA investigators determined that Atlantis
processing could have been expedited with no skipped safety checks for a
February 10 launch. Hence if nothing went wrong there was a five day
overlap for a possible rescue.
Repair
NASA investigators determined on-orbit repair by the shuttle astronauts
was possible but risky, primarily due to the uncertain resiliency of the
repair using available materials.
Columbia did not carry the Remote Manipulator System which would normally
be used for camera inspection or transporting a spacewalking astronaut to
the wing. Therefore an unusual emergency EVA would have been required.
While there was no astronaut EVA training for manoeuvring to the wing,
astronauts are always prepared for a similarly difficult emergency EVA –
to close the external tank umbilical doors located on the orbiter
underside. During launch these doors are open for the propellant feed
lines from the external tank to supply the main engines in the orbiter
tail. If they fail to close after jettisoning the external tank, it
constitutes a thermal protection breach which would destroy the orbiter
upon re-entry. This requires an emergency EVA to close them manually.
Similar methods could have reached the shuttle left wing for inspection or
repair.
For the repair, astronauts would have to use tools and small pieces of
titanium, or other metal, scavenged from the crew cabin. These heavy
metals would help protect the wing structure and would be held in place
during re-entry by a water-filled bag that had turned into ice in the cold
of space. The ice and metal would help restore wing leading edge geometry,
preventing a turbulent airflow over the wing and therefore keeping heating
and burn-through levels low enough for the crew to survive re-entry and
bail out before landing. Because the NASA team could not verify that the
repairs would survive even a modified re-entry, the rescue option had a
considerably higher chance of bringing Columbia's crew back alive.
The Columbia Accident
Investigation Board
Following protocols established after the
loss of Challenger, an independent investigating board was created
immediately following the accident. The Columbia Accident Investigation
Board, or CAIB, consisted of expert military and civilian analysts who
investigated the accident in great detail.
Columbia's flight data recorder was found near Hemphill, Texas on March
20, 2003. Unlike commercial jet aircraft, the space shuttles do not have
flight data recorders intended for after crash analysis. Rather the
vehicle data is transmitted in real time to the ground via telemetry.
However since Columbia was the first shuttle, it had a special flight data
OEX (Orbiter Experiments) recorder, designed to help engineers better
understand vehicle performance during the first test flights. Even after
these were completed, the recorder was never removed from Columbia, and
was still functioning. It records many hundreds of different parameters
and contained very extensive logs of structural and other data which
allowed the CAIB to reconstruct many of the events during the process
leading to break-up. Investigators could often use the loss of signals
from sensors on the wing to track how the damage progressed. This was
correlated with analysis of debris and tests to obtain a final conclusion
about the probable events.
On July 7, 2003 foam impact tests were performed by Southwest Research
Institute, which used a foam block of similar size, mass and speed to that
which struck Columbia, and it created a hole 41 cm by 42.5 cm (16.1 inches
by 16.7 inches) in the protective RCC panel. The tests clearly
demonstrated that a foam impact of the type Columbia sustained could
seriously breach the protective RCC panels on the wing leading edge.
On August 26, the CAIB issued its report on
the accident. The report confirmed the immediate cause of the accident was
a breach in the leading edge of the left wing, caused by insulating foam
shed during launch. The report also delved deeply into the underlying
organizational and cultural issues that led to the accident. The report
was highly critical of NASA's decision-making and risk-assessment
processes. It concluded the organizational structure and processes were
sufficiently flawed that compromise of safety was expected no matter who
was in the key decision-making positions. An example was the position of
Shuttle Program Manager, where one individual was responsible for
achieving safety, timely launches and acceptable costs, which are often
conflicting goals. The CAIB report found that NASA had accepted deviations
from design criteria as normal when they happened on several flights and
did not lead to fatal consequences. One of those was the conflict between
a design specification stating the thermal protection system was not
designed to withstand significant impact damage and the common occurrence
of impact damage to it during flight. The board made recommendations for
significant changes in processes and culture.
In late July 2003, an Associated Press poll revealed that Americans'
support for the space program remained strong, despite the tragedy.
Two-thirds believed the space shuttle should continue to fly and nearly
three-quarters said that the space program was a good investment. On the
question of sending humans to Mars, 49% thought it was a good idea, while
42% opposed it. Support slipped for sending civilians like teachers into
space with 56% supporting the idea and 38% opposed.

Grid on the floor of the Reusable Launch Vehicle (RLV) Hangar where
workers in the field bring in pieces of Columbia's debris. The Columbia
Reconstruction Project Team attempted to reconstruct the bottom of the
orbiter as part of the investigation into the accident.
